
In recent years, telehealth enthusiasts’ interest has been piqued by the concept of telestenting, wherein a robotic system installed at one hospital but controlled from another is used to implant stents during percutaneous coronary interventions (PCIs). If innovators succeed in ironing out the procedure’s wrinkles, there could be many potential benefits, such as bringing PCI to medically underserved areas and boosting the bottom lines of hospitals and cardiology practices.
“Telestenting is very new and still in its infancy, if that, but it holds a lot of promise,” says Ryan Madder, MD, an interventional cardiologist at Spectrum Health in Grand Rapids, Mich.
In the REMOTE-PCI study, Madder and colleagues found that traditional robotic stenting—where a robotic arm is connected with wires to system controls in the next room—could be completed from a distance of 55 feet (Eurointervention 2017;12:1569-76). In two subsequent experiments, Madder performed what he calls “true telestenting” from a simulated catheterization lab over a wireless connection. In the first experiment, the robotic arm was controlled from 4.6 miles away; in the second, Madder successfully implanted a stent in a pig 103 miles away.
Meanwhile, the Mayo Clinic has partnered with Corindus Vascular Robotics on a multi-phase preclinical study of telestenting using the company’s CorPath GRX System. In December 2018, Tejas Patel, MD, chief interventional cardiologist at Apex Heart Institute in Ahmedabad, India, successfully performed five telestenting procedures. He controlled the system’s robotic arm from a temple 20 miles away in Gandhinagar while another physician remained with the patients at the Apex Heart Institute.
In the robotic stenting scenarios—traditional and telestenting alike—the interventional cardiologist sits at a control console using joysticks to direct the robotic arm and a screen to view the arm’s movements. A bedside unit installed in the location where the stenting procedures take place houses the robotic arm and drive, along with single-use cassettes into which the wires, balloons and stents for each procedure are loaded.
Opportunities in the ‘plus’ column
Telestenting makes sense from a number of standpoints, say Madder and other sources whose institutions have introduced robotic angioplasty and stenting. For starters, they claim, it has the potential to improve access to PCI—and consequently, the quality of cardiac care and patient outcomes—in rural or other medically underserved areas. Madder points out that only 80 percent of U.S. residents live within one hour of a PCI-capable facility; in more sparsely populated states like Alaska, West Virginia and Wyoming, the percentage drops to less than 50 percent (Circ Cardiovasc Qual Outcomes 2012;5[1]:14-20).
“The greater the distance patients must travel for PCI, the greater the risk” in emergency situations, Madder says. By eliminating the need for travel, telestenting will be a way to reduce that risk and potentially save lives, he predicts.
Also in telestenting’s “plus” column is the possibility of new revenue for hospitals, though it’s too early to make projections. Whether and at what rate telestenting will be reimbursed are unknowns. And the capital investment for a robotic system is significant. (Corindus did not respond to requests for a price, but Cliffside Research, an equity research firm, estimates it at $350,000 to $650,000 per unit.) Additional costs include the expenses of setting up a control room for the robotic system and, for some remote sites, interventional cardiology equipment. But for hospitals without PCI capability, there are revenues to be earned from treating patients who otherwise would need to be transferred to other institutions for treatment, sources told CVB.
Another way to leverage telestenting for added revenues could come if telestenting is shown to be effective for applications other than PCI, such as acute stroke and peripheral arterial interventions. Madder believes both are possible.
 Proponents also see telestenting technology as a possible means to eliminate or mitigate situations that could have negative impacts on patient care and finances alike, such as staff shortages. They envision scenarios where “experienced operators can help less experienced operators with angiography, stenting, wiring lesions, etc.,” says Ehtisham Mahmud, MD, chief of cardiovascular medicine, director of the Sulpizio Cardiovascular Center-Medicine and director of car-diovascular angiography and stenting at the University of California San Diego School of Medicine. “They won’t replace the interventional cardiologist, but they can play a role.”
Proponents also see telestenting technology as a possible means to eliminate or mitigate situations that could have negative impacts on patient care and finances alike, such as staff shortages. They envision scenarios where “experienced operators can help less experienced operators with angiography, stenting, wiring lesions, etc.,” says Ehtisham Mahmud, MD, chief of cardiovascular medicine, director of the Sulpizio Cardiovascular Center-Medicine and director of car-diovascular angiography and stenting at the University of California San Diego School of Medicine. “They won’t replace the interventional cardiologist, but they can play a role.”
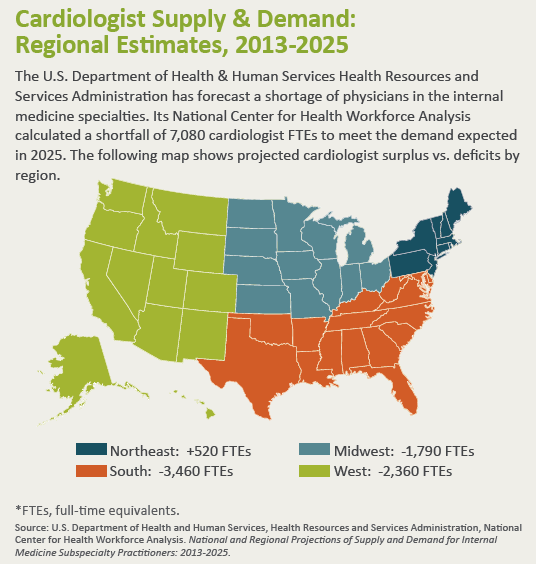
Telestenting “definitely would address the shortage of professionals who can handle PCI cases,” suggests Dipti Itchhaporia, MD, chair of cardiac excellence and medical director of cardiac disease management at the Hoag Heart and Vascular Institute in Newport Beach, Calif. The U.S. Department of Health & Human Services Administration Bureau of Health Workforce has projected a “severe” physician shortage by 2025, including a deficit of about 7,080 cardiologists and hence, a shortage of interventional cardiologists.
Completing the puzzle
Several pieces of the telestenting puzzle must fall into place before it will be ready for prime time. While the results of the telestenting procedures performed in India suggest the concept is clinically viable, many studies—in addition to the one underway at the Mayo Clinic—will be needed to validate the procedure and help experts work through clinical and logistical challenges.
For example, there are technological issues to be sorted out, especially around the wireless network connections necessary to allow remote control of the robotic arm. Latency—the delay between the point at which a command is sent to the robotic arm and the moment the robotic arm begins to follow that command—is a concern, particularly where there is heavy Internet traffic. Anecdotal evidence demonstrates that a latency of up to two seconds was safe for stenting pigs, but whether and how much latency is safe when treating human PCI patients are questions that must be answered, Madder says.
Mahmud concurs. “A second or two of delay may not seem like a big deal but, in this case, it could be,” he insists. “Just as it’s a must to conduct clinical trials of telestenting in general, it’s critical to examine the latency piece.”
Latency may become less of an impediment to telestenting with the advent of 5G networks, which mobile carriers say will offer twice the data transfer speed of the 4G networks now in place in many areas. Spokespersons for AT&T, Sprint, T-Mobile and Verizon told CVB they are developing and testing 5G network technology. AT&T deployed the first mobile 5G network in the U.S. in December 2018, and the availability of 5G mobile networks is expected to increase throughout 2019 and 2020, beginning in major cities. However, as Madder points out, when 5G will be available in remote areas is not known, and general broadband and reliability issues remain a concern in some rural parts of the U.S.
Hospitals that introduce telestenting should expect a steep, but not insurmountable, learning curve, warns Itchhaporia. At the Hoag Heart and Vascular Institute, where the robotic PCI program is in its second year, she has seen “that it takes time and patience to become comfortable with directing and using the technology—but it happens,” she reports. “So, with the right training, there is no reason why a robotic system couldn’t be used for telestenting.”
Researchers and practitioners also will need to reach consensus regarding staffing. Mahmud believes it will always be necessary to have an interventional cardiologist on site to manage possible complications. “As cool as telestenting sounds, without an interventional cardiologist, there is too much of a risk,” he says.
Madder’s not certain the lack of an interventional cardiologist in the room or on the premises would be a deal-breaker for a telestenting program given that an interventional cardiologist will always be the person operating the system controls. Rather, he says, the nonnegotiable requirement might be a skilled individual who has been trained on the robotic system and has experience obtaining vascular access and performing angiography.
“There does need to be someone who can handle complications,” he says. “A non-interventional cardiologist could be a good fit. … It’s important to remember that it’s very, very early days for telestenting. Things will work themselves out in time.”