
At a recent medical conference in Philadelphia, Jennifer Lewey, MD, director of Penn Women’s Cardiovascular Health Program at the Hospital of the University of Pennsylvania, felt deflated when her brief presentation on spontaneous coronary artery dissection (SCAD) generated only a single question from the audience. Her mood changed afterward, when physicians, perhaps embarrassed by their unfamiliarity with the subject, showered her with questions about the subject. “It was an eye-opener for me in terms of getting a sense of the knowledge gaps among general cardiologists, especially providers in the community who are not based at large academic medical centers, about how to diagnose, treat and follow SCAD patients,” she recalls.
Lewey’s experience is a fitting parable for the field’s evolving understanding of a condition long thought to be extremely rare and almost always fatal. A growing body of research and patient advocacy over the past five years has demonstrated that SCAD is more common than originally believed. Current data indicate SCAD may trigger heart attacks in upwards of 35 percent of women under 50 years of age and is the most common cause of myocardial infarction (MI) in pregnant women (Circulation 2018;137:e523-57).
Studies are leading clinicians to evaluate and treat SCAD differently than the atherosclerotic blockages of arteries they were trained to look for. As for survival, the latest clinical data show SCAD to be in the 93 to 98 percent range, according to Sharonne Hayes, MD, professor of cardiovascular medicine at Mayo Clinic in Rochester, Minn. That’s higher, Hayes notes, than the average survival for MI.
As the veil is slowly lifted from SCAD, there’s no denying it is still often under- or misdiagnosed and mismanaged. “I think we’re getting better at looking for [SCAD], but it’s going to take repeated exposure to patients who are not your typical 60-plus male with an elephant on the chest to get it right,” says Malissa Wood, MD, co-director of the Corrigan Women’s Heart Health Program at Massachusetts General Hospital and associate professor of medicine at Harvard Medical School in Boston. “That’s why ongoing training across all avenues is so important in getting doctors and nurses to pay attention when a young person comes into the ER with not-so-typical symptoms.”
Indeed, that unconscious bias of what a heart attack victim looks like helped keep SCAD off the radar screen for so long. “A lot of patients I see with cardiac symptoms were hesitant to seek care in the first place because they felt they wouldn’t be taken seriously,” says Lewey. “So, they often have to become advocates for themselves to get the care and attention they need.” Among the growing field of advocacy and support organizations are the SCAD Alliance, a network of SCAD survivors, researchers and clinicians; SCAD Research, Inc., a volunteer, grassroots group that has raised hundreds of thousands of dollars for research; and WomenHeart, a patient-centered organization that serves women with heart disease.
Another complicating factor has been the difficulties that physicians face in diagnosing the condition since a heart attack caused by SCAD produces the same symptoms as an atherosclerotic MI. Instead, SCAD is a coronary obstruction caused by spontaneous formation of an intramural hematoma within the wall of a coronary artery, or by an intimal tear, which leads to compression of the true lumen and restricted blood flow, triggering MI.
“You really have to have an index of suspicion,” Hayes points out. “One of the challenges is that many of these dissections are in the distal coronary arteries so that people write them off as just a little spasm or as mild coronary disease, when they really demand looking for something that’s a little bit different.”
Multifactorial origins
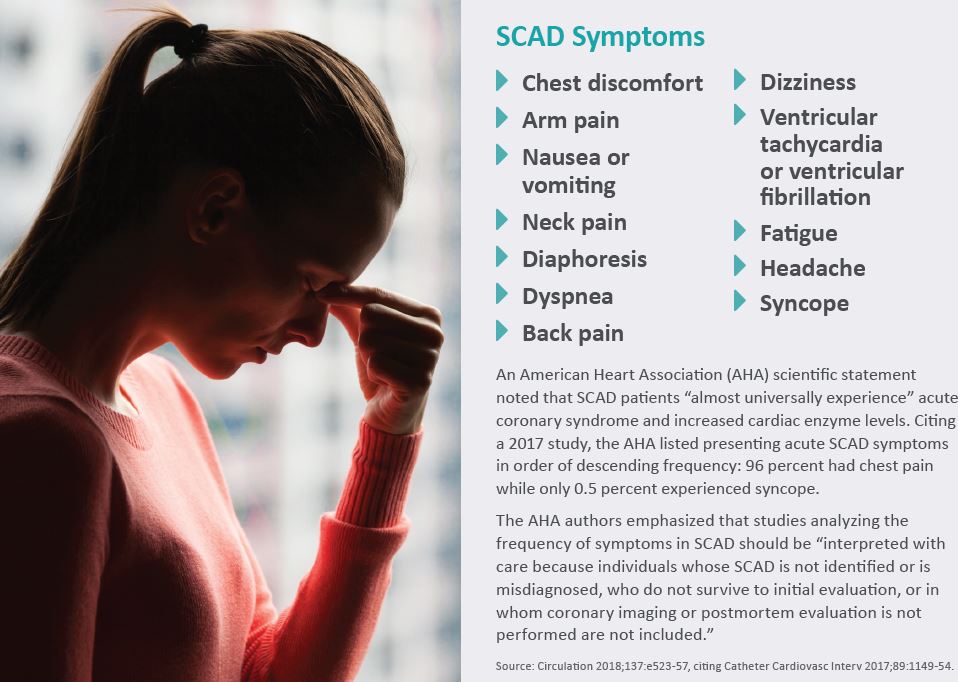
Helping to paint a fuller picture of SCAD is the American Heart Association’s (AHA) first scientific statement on the disease (Circulation 2018;137:e523-57). As spelled out in that report, SCAD may be responsible for up to 4 percent of all acute coronary syndrome cases—though it’s disproportionately higher in young and pregnant women—and is most common among people with few or no traditional cardiovascular risk factors (90 percent of them women).
As for causes, there are plenty of suspects. They include fibromuscular dysplasia (FMD), a non-atherosclerotic vascular disease present in 50 to 70 percent of all patients with SCAD; hormonal influences affecting the arterial walls, which could explain the high SCAD rate in pregnant and postpartum women; and stressors such as extreme physical or emotional stress. Patients who are most susceptible are believed to draw from a combination of these factors. “If someone has multiple risk factors like known FMD or other vascular connective tissue disorders, hypertension, migraine headaches and has had preeclampsia or multiple pregnancies, we definitely recommend that they be followed closely during pregnancy by a [multidisciplinary] team,” says Wood.
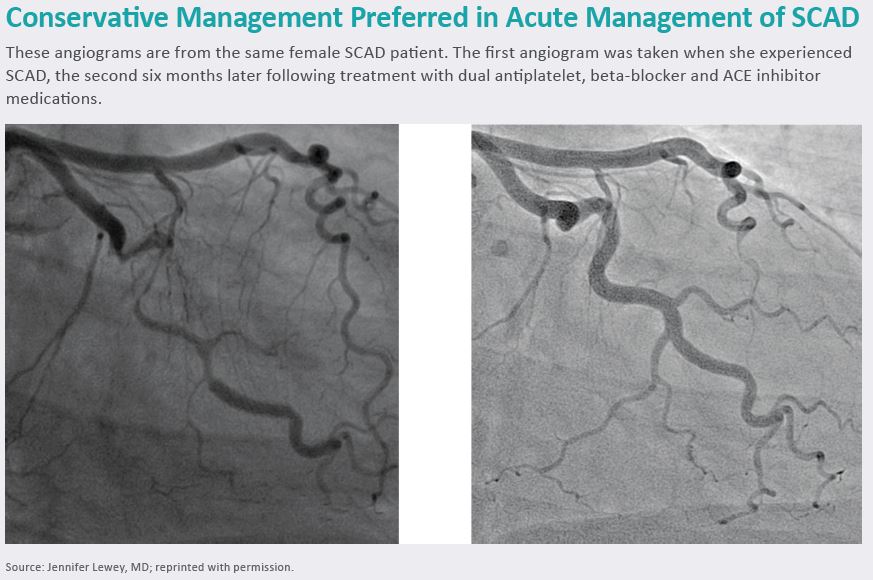
Along with this clearer patient profile have come important new revelations on how to treat patients with SCAD. Research involving 156 patients at Vancouver General Hospital/University of British Columbia found that 86.3 percent of SCAD lesions healed with conservative treatment and that 95 percent of the lesions healed after 30 days according to angiographic findings (JACC Cardiovasc Interv 2019;12[6]:518-27). As accumulating evidence has shown, conservative management translates into a do not stent or pause before you stent approach to SCAD patients who are hemodynamically stable and do not have ongoing ischemia or left main or multivessel proximal dissections.
The AHA’s scientific statement points out that treating SCAD with PCI is associated with an increased risk of complications and suboptimal outcomes caused by introducing guidewires into coronary arteries that are already weak architecturally. The real danger lies in the fact that those guidewires may enter the false lumen created by the spontaneous coronary artery dissection and occlude the true lumen; balloon dilation and stent placement can extend the dissection of the intima or propagate the intramural hematoma upstream and downstream from the vessel, worsening its obstruction.
“What we’ve seen is that dissections heal on their own, sometimes completely, and that patients who get stents can experience worse outcomes,” Lewey sums up. “The message for physicians who treat these patients is that taking a less interventional approach is often the right thing to do.” Medicines like aspirin, beta-blockers and antiplatelet agents also may factor into the regime.
Early imaging is critical
That approach depends on making an accurate diagnosis, and here coronary angiography reigns as the first-line imaging standard for detecting SCAD, largely because of its widespread availability. Intracoronary imaging—including intravascular ultrasound (IVUS) and optical coherence tomography (OCT)—offers even more detailed visualization of the arterial wall and has helped to advance SCAD diagnosis.

These imaging modalities, however, are not without risks, the result again of intrusive guidewires in compromised vessels. But as Hayes—lead author of the AHA scientific statement—notes, the need to use intracoronary imaging has receded in recent years because of improved SCAD-pattern recognition on coronary angiography. “Once people have acquired some experience and are comfortable with the procedure, the need to do IVUS or OCT drops significantly,” she says.
That experience level has grown, especially at academic medical institutions with women’s cardiovascular health centers. These specialized clinics are taking SCAD research and treatment to new levels and, in the process, opening a viable new source of business for hospitals through patient referrals. Mayo Clinic, which paved the way for others by enrolling patients in its SCAD Registry in 2010, is adding around 18 new SCAD patients a month and has treated approximately 500 patients at its Women’s Heart Clinic.
SCAD is leaving its mark on other programs as well, including, for example, Penn Women’s Cardiovascular Health Program, which has seen a steady uptick in SCAD patients while serving as the Philadelphia region’s only referral center for the condition. That program, under Lewey’s leadership, plans to join the iSCAD Registry, launched earlier this year as a multi-center collaborative effort with Boston-based PERFUSE as its coordinating center to advance the pace and breadth of SCAD research around the world. Each month, the Corrigan Women’s Heart Health Program at Massachusetts General sees approximately 15 new SCAD patients from the Boston area and surrounding states. These patients are tended by a 19-member team of specialists that includes general and interventional cardiologists, cardiac nurses, radiologists, a geneticist, a vascular physician as well as behavioral health and cardiac rehabilitation specialists.
“I feel we’re really on an upward trajectory in terms of knowledge acquisition and practice dissemination to colleagues who want to get it right when it comes to recognizing and treating SCAD,” Hayes says. “When you include the tireless work of patient advocates at SCAD Alliance, WomenHeart and SCAD Research, Inc., it’s been something of a perfect storm.”