Proven protocols and practices, people and a push for earlier hemodynamic support are changing the face of cardiogenic shock survival. One leading health system has improved survival rates into the 70+ percent range. And their team believes other facilities should follow suit.
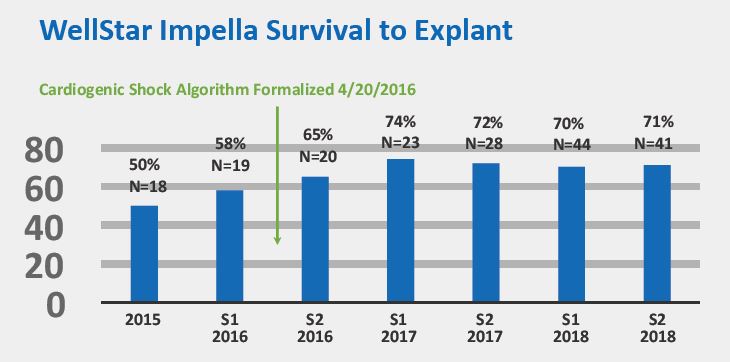
Patient outcomes for acute myocardial infarction cardiogenic shock (AMI-CS) are improving immensely in some health systems, thanks to well-orchestrated, team-based care and advances in early identification and hemodynamic support via a hub-and-spoke model. Well-Star Health System, Georgia’s largest health system, is proof it works: With hub and spoke paired with a proven cardiogenic shock algorithm and best practices, they’ve improved their cardiogenic shock survival from 50 percent, the historical average, to more than 70 percent.
WellStar’s strategy for success—which other health systems can adopt—combines teamwork, rapid response, effective communication and collaboration, physician and administrator champions and consistent 24/7 care across the entire health system.
‘How do we do things better?’
Although incidence of STEMI has declined, the number of cardiogenic shock cases remains stable at approximately 100,000 annually (Circulation 2015;132:1243-51; Health Research International, 2-15). And, after AMI, cardiogenic shock remains the most common cause of in-hospital mortality, with rates exceeding 50 percent.
There are plenty of reasons for the poor outcomes, but even more reasons for physicians, hospitals and health systems to improve them. “Shock is a serious problem that more health systems need to seek effective solutions for,” says Salvatore F. Mannino, DO, MA, FACC, FSCAI, the interventional cardiologist who directs WellStar’s Short-term Mechanical Circulatory Support Program.
“Shock is a team sport,” Mannino quips. “We initially learned that anecdotally through our own patients, but now the evidence proves it unequivocally.”
Too many patients from outside hospitals dying on transfer to the WellStar Kennestone cardiac catheterization lab from other facilities was the motivator for changing the care path at WellStar. “We had to improve patient survival,” Mannino explains. “The sooner these critically ill patients are stabilized, the better they do. So, we sat down with our critical care physicians, cardiac surgeons and critical care cardiologists and asked, ‘How do we do things better?’”
Getting started
Better was a new model, and it didn’t take long to prove itself.
In March 2016, WellStar implemented the hub-and-spoke model, with Mannino at the helm and a cardiogenic shock algorithm that includes temporary hemodynamic support primarily with the Impella CP® heart pump (Abiomed). Well-Star Kennestone Regional Medical Center in Marietta, Ga., served as the hub—the logical choice based on its high volume of cardiogenic shock patients, experience in caring for about 250 STEMIs annually and the availability of 24-hour cardiology critical care expertise, cardiac surgery and advanced heart failure therapies for patients in need of more advanced care. It’s also one of busiest ERs in the country.
Over the ensuing year, WellStar’s other six PCI hospitals deployed this integrated, patient-centered approach to care coordination and delivery.
A multidisciplinary team empowered at every level brings together timely diagnosis, structured protocols, hemodynamic monitoring and guidance, excellent communication across teams and facilities, and centralized care. Patients move seamlessly between both levels of care and WellStar’s facilities as needed.

WellStar owes some of its rapid success with hub-and-spoke to its experience with the Impella®. The system’s physicians started using Impella 2.5® in 2012. Two years later, Mannino learned that AMI-CS patients treated with Impella pre-PCI combined with a team approach to care had better outcomes. In 2016, an FDA premarket approval expanded Impella CP use to include AMI-CS patients. WellStar followed suit, with convincing results. “Better outcomes in using Impella in two or three shock patients is all it took for us to turn around our thinking,” Mannino says. That was the jumping-off point for Mannino and his team to develop an algorithm to improve the care of AMI-CS patients.
The key, they realized, was building a team-based program around early restoration of favorable hemodynamics coupled with complete revascularization. “Our group did some research and literature searches on the optimal strategy for heart support and adopted the programmatic approach to AMI-CS care introduced by Dr. Bill O’Neill in Detroit,” Mannino recalls. “It was anecdotal evidence at the time, but it was a big move in the right direction. Our timing was very much in parallel with his team.” 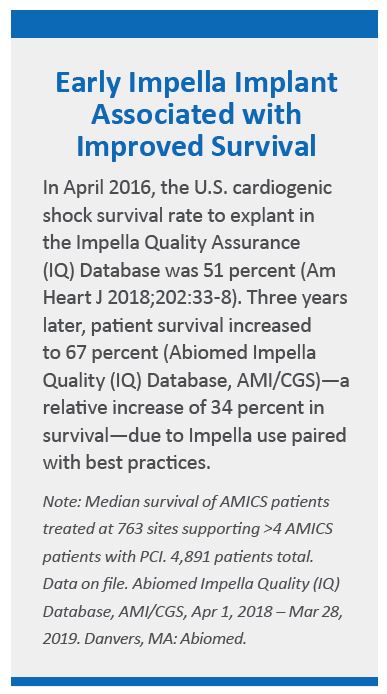
Over a couple months, Mannino and a clinical team built their algorithm based on current best practices. Physicians, nurses, care coordinators and emergency transporters from the health system received training via a comprehensive program created by Abiomed for managing and transferring shock patients with Impella. Teams are trained and guided by algorithms for shock identification, treatment, escalation, weaning and transfer. Step-by-step tools and checklists support the care team when a patient with an Impella is moved from a spoke to a hub hospital.
The teams tested and refined the protocol at Kennestone Hospital, their tertiary care center that serves as the hub. When they extended the spokes across the health system, six other PCI hospitals established programs to place Impella.
“Survival is very time-dependent in cardiogenic shock,” Mannino says. “The sooner you treat patients upfront and restore not only myocardial, but tissue, perfusion, the better patients do. The system needed an irreproachable pathway to improve survival in these critically ill patients.”
The hub-and-spoke model was built on best practices and registry data, notably early shock therapy, upfront (pre-PCI) use of Impella CP, complete coronary revascularization and right heart catheterization in all patients, as well as minimizing the use of toxic inotropes and vasopressors. They also deployed best practices for safe vascular access, utilizing micropuncture and ultrasound guidance, along with mandating the use of vascular closure devices.
Teams work
Teamwork is central to WellStar’s good outcomes. Across the health system, teams have learned to identify cardiogenic shock patients at a critical early stage. They optimize patient access and elevate patients to an appropriate level of care at an appropriate facility. Most often that means inserting an Impella pre-PCI and performing percutaneous revascularization prior to transporting the patient to Kennestone, where they receive 24/7 high-level care from experienced physicians, advanced practitioners and cardiac critical care nurses.
At Kennestone, multidisciplinary rounds are performed twice daily. Rounds generally include an intensivist, critical care cardiologist, advanced practitioners, nutritionists, pharmacists, care coordinators and, when needed, advanced heart failure specialists and structural heart specialists.
“We have very layered rounds on these patients with a well-thought-out game plan for further escalation and de-escalation,” Mannino says. “Treatment of heart failure or shock is not solely device therapy. It’s a pathway for treatment. And care must be high quality 24/7. That is why we have a hub hospital readily available that brings that very high-level care.”
WellStar made a point of baking other essential ingredients into its algorithm: nonstop communication, collaboration and making everyone on the team feel their input is valid and important. “The more you educate and communicate, the more success will come,” Mannino explains. “You need physician champions paired with administrator champions to make this work well. You need to have barrierless communication as each one’s input is uniquely vital to the outcome of the patient.”
Despite the talk of ingredients, Mannino emphasizes that his team’s algorithm-based hub-and-spoke model is playbook medicine, not cookbook medicine. Success doesn’t come from following a recipe. “An algorithm should never supplant sound clinical judgment,” he insists. “The algorithm is a guide to therapy, not a mandate. We say playbook because at times we have to go audible like they do in football. Sometimes you have to side-step and individualize the right device and pathway for the patient.”
Post-discharge care is a key element to good outcomes, too. High-risk patients, especially those with a severely reduced ejection fraction, are referred to the Comprehensive Care Clinic, where they are closely followed by advanced heart failure physicians, advanced practitioners, comprehensive care specialists (nutrition, cardiac rehab, pharmacists) and, if needed, electrophysiologists. “We’re very deliberate in how we individualize treatment of these patients,” Mannino says. “The meticulous care does not end once the patient is discharged. It’s full-circle care.”
The numbers prove it
When WellStar rolled out its hub-and-spoke model, its AMI-CS survival was at about 50 percent, consistent with national averages. Within a few months, survival rates soared through the 60s and into the mid-70s, which is consistent with new national averages for centers that have adopted similar best practices.
Data presented and published in May 2019 from the National Cardiogenic Shock Initiative Study (NCSI)—on 171 consecutive AMI-CS patients from 35 sites—shows 72 percent survival with 98 percent native heart recovery at discharge. Those patients were treated with the NCSI protocol, which includes Impella placement before revascularization. The study, published in May in Catheterization and Cardiovascular Interventions, also demonstrated that a protocol-based approach to increasing survival rates in cardiogenic shock is reproducible in academic and community hospitals across the U.S.
“NCSI shows us that it’s upfront use and early therapy that’s best for these patients,” Mannino says. “It’s helping usidentify which patients would do well. It’s more proof that this works. More health systems need to be doing this.”
Across the U.S., there’s a lot of room for growth. Currently only about 10 percent of patients with shock are supported pre-PCI via Impella. “It would be great if everyone in shock presented to a high-volume shock center, but most do not,” Mannino says. “This model, if extended to more hospitals, would dramatically impact the likelihood of survival and heart recovery with a good quality of life after discharge.”
![]() Guiding growth
Guiding growth
Today, WellStar is seeing more patients than ever. Across the health system, they’re recognizing shock earlier. And more outside referrals are coming from other institutions, in Atlanta and from neighboring states. WellStar has grown from a cardiogenic shock program caring for its local community to a recognized shock referral center.
“We have patients being transferred to us from outside hospitals and health systems, some even larger in size, because of a growing confidence in the care we provide and the outcomes we have demonstrated,” Mannino notes. “We’re glad to take care of these patients, but we’d also be glad to see other facilities adopting the strategies we have to help shock patients. It is very doable from the clinical and administrative levels.”
Mannino is confident his team can handle their growing numbers. “We have had tremendous saves with the use of Impella,” he says. “Success to me is sending a patient home with his or her native heart to have a functional life. Survival is one goal, but native heart recovery is our endeavor. That is why we embarked on this project.”
Important Risk Information for Impella devices
INDICATIONS FOR CARDIOGENIC SHOCK
The Impella 2.5®, Impella CP®, Impella CP® with SmartAssist®, Impella 5.0® and Impella LD® Catheters, in conjunction with the Automated Impella® Controller (collectively, “Impella® System Therapy”), are temporary ventricular support devices intended for short term use (≤ 4 days for the Impella 2.5, Impella CP, and the Impella CP with SmartAssist, and ≤ 14 days for the Impella 5.0, and Impella LD) and indicated for the treatment of ongoing cardiogenic shock that occurs immediately (< 48 hours) following acute myocardial infarction or open heart surgery or in the setting of cardiomyopathy, including peripartum cardiomyopathy, or myocarditis as a result of isolated left ventricular failure that is not responsive to optimal medical management and conventional treatment measures (including volume loading and use of pressors and inotropes, with or without IABP). The intent of Impella System Therapy is to reduce ventricular work and to provide the circulatory support necessary to allow heart recovery and early assessment of residual myocardial function.
CONTRAINDICATIONS
The Impella 2.5, Impella CP, Impella CP with SmartAssist, Impella 5.0 and Impella LD are contraindicated for use with patients experiencing any of the following conditions: Mural thrombus in the left ventricle; Presence of a mechanical aortic valve or heart constrictive device; Aortic valve stenosis/calcification (equivalent to an orifice area of 0.6 cm2 or less); Moderate to severe aortic insufficiency (echocardiographic assessment graded as ≥ +2); Severe peripheral arterial disease precluding placement of the Impella System; Significant right heart failure*; Combined cardiorespiratory failure*; Presence of an Atrial or Ventricular Septal Defect (including post-infarct VSD)*; Left ventricular rupture*; Cardiac tamponade* * This condition is a contraindication for the cardiogenic shock indication only.

Mary joined TriMed Media in 2003. She was the founding editor and editorial director of Health Imaging, Cardiovascular Business, Molecular Imaging Insight and CMIO, now known as Clinical Innovation + Technology. Prior to TriMed, Mary was the editorial director of HealthTech Publishing Company, where she had worked since 1991. While there, she oversaw four magazines and related online media, and piloted the launch of two magazines and websites. Mary holds a master’s in journalism from Syracuse University. She lives in East Greenwich, R.I., and when not working, she is usually running around after her family, taking photos or cooking.